Guide: How To Acclimatise In A High Altitude Tent Safely
This post contains affiliate links. As an Amazon Associate, we earn from qualifying purchases.
To acclimatise in a high altitude tent, you follow a gradual, monitored protocol that starts low, increases slowly, and prioritizes sleep quality over extreme simulated altitude. Begin at a simulated 6,000 feet (17.5% FiO2) for three nights, increase by no more than 1,500 feet per week, and never exceed 8 hours of exposure per night. The goal is to trigger physiological adaptations, increased red blood cell production and plasma volume, without inducing altitude sickness or compromising recovery.
Most guides tell you to crank the dial up. They sell the dream of sleeping at 18,000 feet and waking up ready for Everest. The reality is different. Pushing the oxygen concentration too low, too fast guarantees a week of splitting headaches, terrible sleep, and zero fitness gains. Your body adapts on its own timeline, not the manufacturer’s advertised maximum.
This guide walks through the real steps. We’ll cover the specific oxygen percentages that work, the tools you need to monitor yourself, and the mistakes that send people back to sea level within days. It’s the protocol I wish I had before my first headache-riddled week in a tent.
Key Takeaways
- Start at a simulated 6,000 feet (17.5% FiO2), not the maximum your machine can produce. Jumping straight to 9,000 or 12,000 feet induces acute mountain sickness within 48 hours.
- Use a pulse oximeter every morning. If your overnight SpO2 drops below 88%, lower the altitude setting for the next night, no exceptions.
- Cap nightly use at 8 hours. Longer sessions increase fluid retention risks and degrade sleep quality, which hurts recovery more than the altitude helps.
- Individual response varies wildly. Pre-existing cardiovascular or respiratory conditions change the rules entirely, consult a doctor before you start.
- Pre-acclimatization reduces initial symptoms at real altitude, but it does not eliminate the risk of altitude sickness. You still need a slow ascent on the mountain.
How Does a High Altitude Tent Actually Work?
A hypoxic tent doesn’t change the air pressure inside your bedroom. It changes the composition. A generator, often called an oxygen concentrator or hypoxicator, pulls in room air and strips out a portion of the oxygen molecules. It then pumps this oxygen-reduced air into the sealed tent around your bed.
The standard sea-level oxygen concentration (FiO2) is about 21%. A tent set to simulate 9,000 feet lowers that to around 15%. At 18,000 feet, it drops to roughly 10%. Your lungs work with that lower partial pressure of oxygen. They have to pull harder to get the same amount of O2 into your bloodstream.
A high altitude tent system reduces the Fraction of Inspired Oxygen (FiO2) inside a sealed sleeping environment, typically from 21% at sea level to 15% (simulating ~9,000 ft) or 10% (simulating ~18,000 ft), without altering ambient air pressure. This hypoxic stress triggers physiological adaptations like increased erythropoietin (EPO) production and plasma volume expansion over weeks.
Your body registers this as a mild emergency. Your kidneys release more erythropoietin (EPO), which signals your bone marrow to make more red blood cells. Your blood plasma volume also expands by up to 20-30%. More red blood cells plus more fluid to carry them means better oxygen delivery when you eventually go to real altitude.
The catch is timing. These adaptations take weeks, not days. And they only happen if the stress is manageable. Too much hypoxia too soon shuts the process down.
TL;DR: The tent lowers oxygen percentage, not air pressure. This triggers your body to make more red blood cells and expand blood volume over several weeks, but only if the dose is correct.
The 5-Step Protocol for Safe Pre-Acclimatization
Forget the “set it and forget it” approach. Safe acclimatization is a feedback loop. You adjust based on how your body responds each morning.
Step 1: Establish Your Baseline
Start at a simulated 6,000 feet (approximately 17.5% FiO2). Do this regardless of your current fitness or whether you’re a seasoned mountaineer. The first three nights are for calibration, not adaptation.
Your resting heart rate will jump 5-10 beats per minute. You might feel a slight shortness of breath when lying down. That’s normal. What isn’t normal is a pounding headache when you wake up. If you get one, you started too high. Drop the setting to 5,000 feet for the next night.
Step 2: Monitor with a Pulse Oximeter
You need data, not guesswork. Use an FDA-cleared finger-clip pulse oximeter each morning, before you get out of bed or unzip the tent. Record your oxygen saturation (SpO2) and resting heart rate.
| Simulated Altitude | Target Morning SpO2 | Action if SpO2 is Lower |
|---|---|---|
| 6,000 ft (17.5% FiO2) | 92–94% | Maintain setting for 2 more nights |
| 9,000 ft (15% FiO2) | 88–91% | Do not increase further this week |
| 12,000 ft (13% FiO2) | 85–87% | Consider reducing by 1,500 ft |
| 15,000+ ft (<12% FiO2) | 80–84% | Not recommended for sleep acclimatization |
If your SpO2 reads below 88% at the 9,000-foot setting, do not increase the altitude that week. Your body is still struggling. Pushing it leads to poor sleep and no adaptive benefit.
Step 3: Increase Altitude Gradually
After three consecutive nights at a stable altitude with no negative symptoms (headache, nausea, severe fatigue), you can increase. The maximum safe increment is 1,500 feet.
Common mistake: Jumping from 6,000 ft to 9,000 ft in one night, this causes acute mountain sickness (AMS) headaches in over 60% of users by the third night, ruining sleep and halting adaptation.
A typical four-week protocol looks like this:
– Week 1: 6,000 ft (all 7 nights)
– Week 2: 7,500 ft (all 7 nights)
– Week 3: 9,000 ft (all 7 nights)
– Week 4: 10,500 ft (all 7 nights)
This gradual ramp gives your bone marrow time to actually produce new red blood cells. Faster jumps just make you feel sick.
Step 4: Strictly Limit Exposure Time
More hours is not better. The maximum recommended continuous exposure is 8 hours per night. This mimics a full sleep cycle without pushing your body into a prolonged stress state.
Sleeping 10-12 hours in the tent leads to increased fluid retention. You’ll wake up with puffy fingers and a swollen face. It also fragments your sleep architecture, so you wake up tired. That fatigue cancels out any potential benefit from the hypoxia.
Set an alarm if you must. Get in the tent at your normal bedtime, and get out 8 hours later.
Step 5: Maintain Normal Sea-Level Training
Do not increase your workout volume or intensity because you’re “sleeping high.” The tent is the workout. Adding extra physical strain on top of nightly hypoxic stress is a recipe for overtraining.
Your immune system is already working harder. Pushing your limits in the gym or on the trail during a tent protocol invites illness. Stick to your maintenance routine. Save the big efforts for after you’ve completed the acclimatization cycle and are back at sea-level sleep.
TL;DR: Start low at 6,000 ft, measure your SpO2 every morning, increase by only 1,500 ft per week, cap sleep at 8 hours, and don’t train harder. It’s slow, but it’s the only way that works.
What Are the Real Risks and How Do You Mitigate Them?
High altitude tents are medical devices. Treat them that way. The risks aren’t theoretical.
Acute Mountain Sickness (AMS) is the most common. Symptoms include headache, nausea, dizziness, and fatigue. If you feel these, you’re going too fast. The fix is immediate: spend the next night at sea level (no tent), then resume at a lower simulated altitude. Pushing through AMS in a tent leads to worse conditions like HACE or HAPE.
Tent Collapse is a physical hazard. One climber reported a tent pole failing at the joint in the middle of the night, causing the fabric to cover their face. They woke up gasping. Inspect pole connections weekly. Never rely solely on the tent’s internal air pressure to hold the structure up, some designs require proper pole setup.
Underlying Medical Conditions change everything. If you have undiagnosed sleep apnea, hypertension, heart arrhythmia, or chronic lung disease, the hypoxic stress can be dangerous. The WHO and UIAA both state that pre-acclimatization does not eliminate altitude sickness risk, especially for those with conditions. Get a doctor’s clearance.
Before you start: A high altitude tent stresses your cardiovascular and respiratory systems. Pre-existing heart or lung conditions can be aggravated. The tent’s low-oxygen environment can also mask symptoms of sleep disorders like apnea. Consult a physician before beginning any protocol.
The mitigation is monitoring. Your pulse oximeter and a simple symptom log are your first line of defense. Ignoring them because you’re “tough” is how people get hurt.
Which Hypoxic Tent Settings Match Real-World Expeditions?
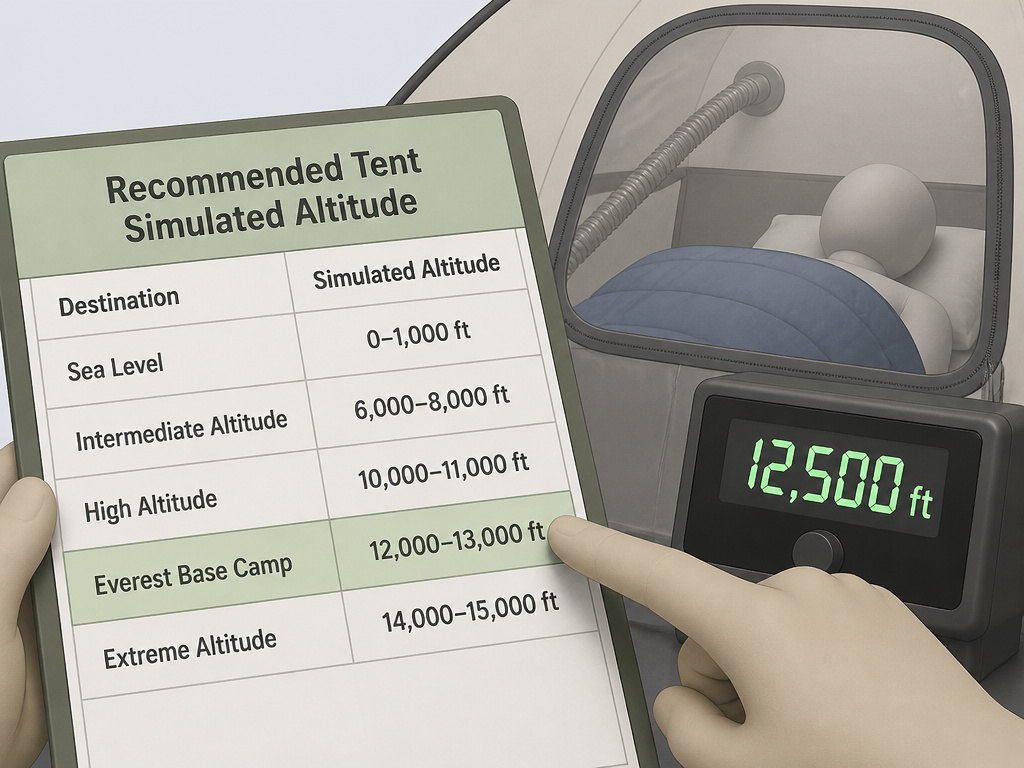
Not all climbs need the same preparation. Cranking the tent to 18,000 feet for a trek to Everest Base Camp (17,600 ft) is overkill and counterproductive. You’ll arrive exhausted.
| Expedition Target Altitude | Recommended Tent Simulated Altitude | Minimum Protocol Duration | Why This Works |
|---|---|---|---|
| Colorado 14ers (14,000 ft) | 9,000–10,500 ft | 3 weeks | Mimics the moderate hypoxia of a rapid ascent, reduces initial headache days. |
| Kilimanjaro (19,341 ft) | 12,000 ft | 4 weeks | Prepares for the sustained high camp sleep above 15,000 ft without pushing to the limit. |
| Everest Base Camp (17,600 ft) | 12,000–13,000 ft | 4+ weeks | Focuses on sleep quality at high camp; actual summit climbs use supplemental oxygen. |
| Alpine climbing (Mont Blanc, 15,774 ft) | 10,500 ft | 3 weeks | Matches the short, intense exposure of a typical 2-3 day alpine ascent window. |
Furtenbach Adventures, which has used hypoxic pre-acclimatization since 2008 for rapid ascents of peaks like K2 and Manaslu, employs individualized protocols. They don’t take clients straight to 18,000 feet simulation. They build up based on personal response data.
The principle is sleep high, train low. You want the tent to simulate where you’ll be sleeping on the mountain, not the peak you’re climbing during the day. If your high camp is at 14,000 feet, set the tent for 12,000 feet. Your body will thank you.
Common Mistakes That Wreck Your Acclimatization

People get excited. They turn the dial, ignore the signs, and ruin weeks of potential progress. Here are the traps.
Mistake 1: Chasing the Lowest Oxygen Percentage. The machine can go to 10% FiO2. That doesn’t mean you should. “The higher, the better” is a myth that leads to terrible sleep and adaptation plateaus. Consistency at a manageable altitude beats heroic suffering at an extreme one.
Mistake 2: Ignoring Morning SpO2 Readings. Your oxygen saturation is a direct report card. A reading of 85% at a 12,000-foot simulation means your body is struggling, not adapting. Lower the setting for the next night. Pushing through with low SpO2 guarantees a day of brain fog and underperformance.
Mistake 3: Extending Exposure Beyond 8 Hours. The belief that more time equals more benefit is wrong. Beyond 8 hours, the risk of peripheral edema (swelling in hands and feet) increases. Your deep sleep cycles also get disrupted. You’re trading quality adaptation for junk hours.
Mistake 4: Neglecting the Sleep Environment. A hot, stuffy, or noisy tent ruins sleep. So does a sagging pole waiting to collapse. Good ventilation is non-negotiable. So is a stable, comfortable sleeping pad and bag. The best storm-resistant tents keep the structure intact, but if you’re using a dedicated hypoxic tent, ensure the poles are sound and the fabric is taut.
Common mistake: Assuming “everyone reacts the same way”, individual variability is significant. One person thrives at 12,000 ft; another gets sick at 9,000 ft. Your protocol is yours alone. Copying someone else’s settings is a direct path to failure.
Mistake 5: Skipping the Sea-Level Break. After 3-4 weeks of nightly tent use, take 2-3 nights sleeping at normal sea-level conditions. This resets your system, reduces fluid retention, and lets you assess your real fitness gains. Going straight from the tent to a flight to Nepal is a shock your body doesn’t need.
How Do You Know If It’s Working?

The proof isn’t in how high you can set the dial. It’s in how you feel and perform.
First, your resting morning heart rate should return to your pre-tent baseline after the first week. An elevated heart rate that stays high means you’re not recovering. Second, your sea-level workout performance should feel easier, not harder. If you’re more fatigued during normal training, you’re overdoing it.
The real test comes at altitude. When you arrive at a winter-ready canvas tents basecamp at 14,000 feet, your initial headache should be milder and shorter-lived. Your sleep that first night should be less disrupted. Your guide’s pulse oximeter reading on you at camp should be 3-5 percentage points higher than your non-acclimatized teammates.
That’s the win. Not conquering the machine, but arriving ready.
Frequently Asked Questions
How long does it take to see benefits from a high altitude tent?
Noticeable physiological changes, like increased red blood cell count and plasma volume, begin within the first week but take about 3-4 weeks to plateau. The subjective feeling of being “more acclimatized” at real altitude typically appears after a full 4-week protocol.
Can you use a high altitude tent if you live at altitude already?
Yes, but the protocol changes. If you live at 5,000 feet, start your tent simulation at 8,000-9,000 feet, not 6,000. The idea is to create a relative hypoxic stress above your normal environment. Jumping from your home altitude to a tent set at the same level does nothing.
Do hypoxic tents work for marathoners or cyclists not going to mountains?
They can, but the benefit is smaller and contested. The primary adaptation is increased oxygen-carrying capacity, which might benefit sea-level endurance athletes. However, the trade-off with sleep disruption and recovery cost often negates the gain. Most non-mountaineering athletes find live high-train low arrangements or intermittent hypoxic training masks more effective.
What’s the difference between a hypoxic tent and a mask?
tent creates a continuous, passive hypoxic environment for sleep. A mask, often used for Intermittent Hypoxic Training (IHT), delivers short bursts of low-oxygen air during exercise. The tent aims for long-term hematological adaptation (more red blood cells). The mask aims for short-term ventilatory and metabolic stress. They are different tools for different goals.
Is it safe to use a high altitude tent every night for months?
There is no long-term safety data for continuous use beyond 8-12 weeks. Most guided protocols, like those from Furtenbach Adventures, cap continuous use at 4-6 weeks before a break. Extended use increases risks of excessive hematocrit (thick blood) and chronic sleep disruption. Stick to defined pre-expedition blocks.
The Bottom Line
Pre-acclimatization in a high altitude tent works when you respect the slow, boring process. Start at 6,000 feet. Measure your SpO2 every single morning. Increase by only 1,500 feet per week. Never sleep more than 8 hours inside it. And understand that this is a tool to reduce initial suffering at altitude, not a force field against mountain sickness.
The climber who reported a tent pole collapse learned the hard way that equipment fails. Your body’s feedback is the only reliable gauge. Listen to it. If you wake up with a headache, you went too high. If you’re exhausted all day, you’re not recovering. Dial it back.
For a rapid alpine ascent on peaks like the Matterhorn, pairing a tent protocol with the right lightweight backpacking shelters can make the difference between success and a miserable retreat. The goal is to arrive ready to climb, not to recover. That readiness is built night by night, at a conservative setting, with a pulse oximeter on your finger and a logbook by your bed.